Because anti-oppression efforts cannot be effective unless we all have a shared understanding of what is being discussed, the current definition will be provided to deepen our practice healing and repair.
What is Privilege?
The definition of privilege, as used in critical race theory and anti-oppression work, was coined in 1988 by a women’s-studies scholar at Wellesley by the name of Peggy McIntosh.
McIntosh defined the term ‘privilege’ as:
unearned advantage (based upon race, class, religion, ethnicity, sexual orientation, age or ability) which can be observed both systemically and individually.
McIntosh, Peggy. White Privilege and Male Privilege: A Personal Account of Coming to See Correspondences Through Work in Women’s Studies. Wellesley, MA: Wellesley College, Center for Research on Women, 1988. Print.
Although McIntosh originally used the term to describe implicit bias and advantages given on the basis of race and gender (particularly whiteness and maleness), systems of privilege exist across numerous demographic categories:
For example, income based privilege affords social, political, and economic advantages to those who have a higher income or concentration of wealth than it does to someone from a low-to-moderate income background. In fact, those living in poverty have higher rates of death and illness, are more likely to remain in poverty, and have poor access to social determinants of health like quality schools, jobs, food, transportation, neighborhood amentities, etc.
“We live in a culture that affirms privilege, dominant culture, and supremacy. Most people in the privileged group have no awareness of their capacity to move in space freely because of how privilege operates in culture. Privilege is constructed for social and political reasons. It has changed over time based upon the goals of supremacy, divide and conquer. Privileged attributes give privileged people a pass.
A lack of awareness on the privileged person’s part about their privilege within a cultural context, allows for them to be willfully ignorant and to have the privilege of being resistant to the idea that they are in a system that erroneously teaches them that they are on a level playing field with those who aren’t afforded access to the same privileges.
Privilege derails work toward liberation and justice because people who experience privilege can stay in a space of being defensive while people without access to those advantages are struggling to survive and to respond toward a system that is designed to annihilate them.” ~ Michelle C. Johnson Paraphrased
Johnson’s work explicitly describes the role of ‘whiteness’ as a construct which strips communities of color of their capacity to:
define their own reality (due to the influence of dominant narratives)
play on a level playing field (as often groups without access to resources rarely start at the same place as someone born to advantages or even know/ have access to the rules of the game)
encounter messages that don’t instill myths of inferiority or that they aren’t worthy of investment and care
receive a fair opportunity to secure living wage jobs, bank loans, quality education, healthy housing and amenities, etc.
visibility
credibility
perception of worth
But the concepts can apply to a myriad of other categories in which privilege has created individual and systemic harm.
Including faith tradition, biological sex, level of educational attainment, whether or not you have a disability, speak English as a first language, sexual orientation, age, gender identity, and citizenship status.
Johnson uses the topic of privilege in her book to deepen the discussion around healing and repairing historical harm to encourage us to mindfully consider which identities we possess and how we are either afforded privileges or may be targeted because of those identities.
Guided Activity
How does privilege or oppression show up?
For example:
Identities
Black
Targeted by historical trauma, past & current policies/ institutional practices that limit access to resources, implicit biases, etc.
Woman
Targeted by historical trauma, past & current policies/ institutional practices that limit access to reproductive rights, wage parity, etc.
College graduate
Experience privilege in form of access to better paying jobs and a livable wage than someone without a degree.
To learn more about Johnson’s efforts to help those who have benefitted from and been harmed by privilege heal, check out her Insta:
According the Centers for Disease Control, a legislative agenda is a policy development strategy designed to prevent injury and the spread of illness/ disease by conducting health and economic analysis of the burden by injuries and their consequences that should be voted upon by state, local, and federal legislators (1). The legislative agenda is used to estimate how much evidence-based prevention will be needed to avert healthcare costs from an organizational, public health, or societal perspective.
Why would you need a legislative agenda?
The following public health policy priorities listed below are provided to demonstrate how you can advocate for an issue that you care about [in collaboration with social justice advocates, health providers, and philanthropic organizations].
Action Plan Template [part 1]
This Legislative Agenda [template] lists objectives for legislative action at the national level on Mental Health Reform issues that affect the quality of care patients receive when seeking mental health services, including instances in which the patient has been ordered to receive involuntary care.
The agenda was created to demonstrate the process of identifying high-priority issues for legislative action and to create a business case for better coordination of care when regulatory action is needed.
In addition to the legislative priorities for advocacy, the issues identified in the template also create a business case for the creation of an augmented reality app which helps patients provide informed consent/ monitor whether they are receiving humane care and assists patients with tracking medical information including:
In this action plan template, we will first list national level policies that should be followed and monitored by mental health providers that should be reported to the following agencies when they are not adhered to. We will also list the following forms of documentation you should/ and can request to receive when seeking mental health care.
Second, we will identify key issues that may emerge while seeking mental health care at the state, regional, or local level and for which effective patient advocacy may be compromised due to lack of coordination and a lack of regulation regarding informed consent, and recommendations for how to address these challenges.
Note: don’t hesitate to use you resources including your local health department, primary care provider, legal aid, or philanthropic institutions.
This post is under construction.
Key Terms and Concepts:
Although health practitioners often refer to the following health care terms as if they are interchangeable, it’s important for those seeking medical care and patient advocates to understand the differences between the following concepts in order to receive the appropriate care:
Mental Health: According to the Centers for Disease Control [CDC],
Mental health is an important part of overall health and well-being (2). Mental health includes our emotional, psychological, and social well-being. It affects how we think, feel, and act. It also helps determine how we handle stress, relate to others, and make healthy choices.
Behavioral Health: According to the Substance Abuse and Mental Health Services Administration [SAHMSA],
Behavioral health refers to the evidence-based interventions for disruptive behavior disorders and diagnostic categories or behaviors that cause trouble at home, school/work, or in the community at-large (3).
Behavioral disorders may involve (4):
Inattention
Hyperactivity
Impulsivity
Defiant behavior
drug use
criminal activity
Such behavior may first appear in any developmental stages: early childhood, school age, or adulthood (3).
Disability: The World Health Organization defines the term ‘Disability’ as:
an umbrella term for impairments, activity limitations and participation restrictions, referring to the negative aspects of the interaction between an individual (with a health condition) and that individual’s contextual factors (environmental and personal factors)(5)
which require specific health, educational, rehabilitation, social, and support needs (6).
Disability is measured and assessed by the individual’s ability to capacity to navigate their own health conditions, environmental factors, and functional daily activities with little or no impediments (7).
Mental Illness: The Substance Abuse and Mental Health Services Administration defines mental illness as:
Mental disorders that involve changes in thinking, mood, and/or behavior (8). These disorders can affect how we relate to others and make choices. These illnesses are common, recurrent, and often serious, but they are treatable and many people do recover.
Serious mental illness is defined by someone over 18 having (within the past year) a diagnosable mental, behavior, or emotional disorder that causes serious functional impairment that substantially interferes with or limits one or more major life activities.
For people under the age of 18, the term “Serious Emotional Disturbance” refers to a diagnosable mental, behavioral, or emotional disorder in the past year, which resulted in functional impairment that substantially interferes with or limits the child’s role or functioning in family, school, or community activities.
Trauma: According to The Substance Abuse and Mental Health Services Administration,
Individual trauma results from an event, series of events, or set of circumstances experienced by an individual as physically or emotionally harmful or life-threatening with lasting adverse effects on the individual’s functioning and mental, physical, social, emotional, or spiritual well-being (9).
Substance Use Disorder: According to The Substance Abuse and Mental Health Services Administration,
Substance use disorders occur when the recurrent use of alcohol and/or drugs causes clinically significant impairment, including health problems, disability, and failure to meet major responsibilities at work, school, or home (8).
In a previous post, we defined the term ‘equity‘ and explained how this indicator for human agency has been historically used to create health and economic disparities.
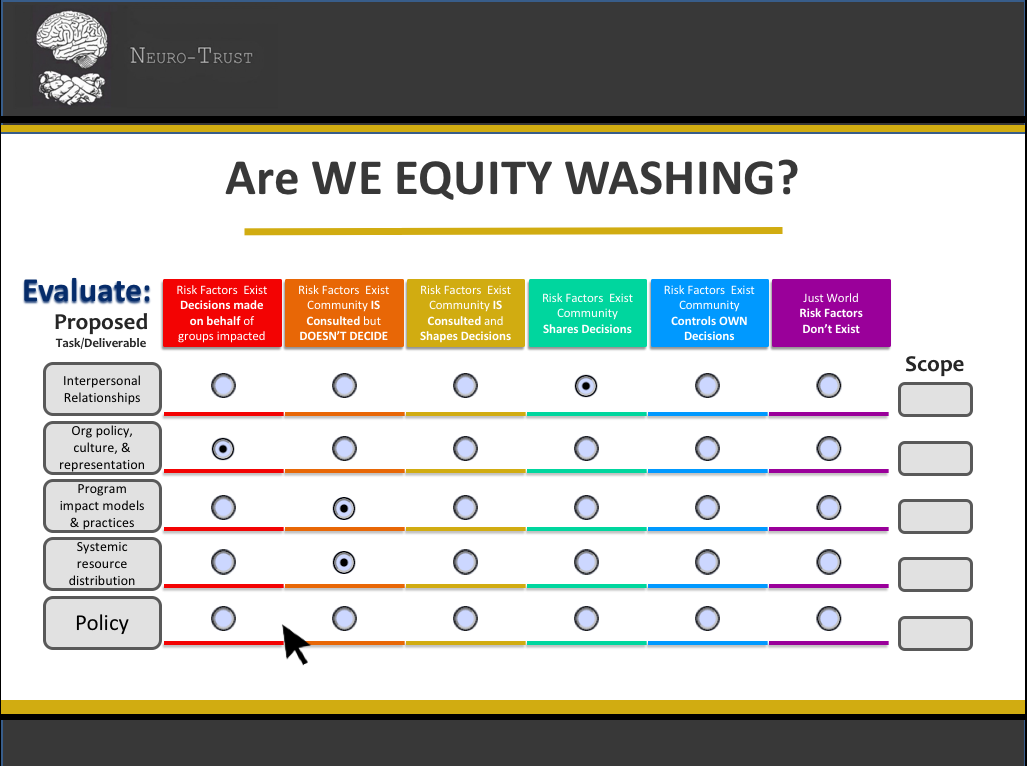
Now that we’ve described the concept of equity and how this assessment indicator is used, we’ll share a rubric that can be used to assess whether you or your organization may be ‘Equity Washing.’
What is ‘Equity Washing?’
If equity is measured by the Centers for Disease Control as
“ …the measurable standard by which every person has the opportunity to “attain his or her full health potential” and no one is “disadvantaged from achieving this potential because of social position or other socially and economically determined circumstances.”
Equity Washing refers to the assessment criteria by which we create barriers (either intentionally or unintentionally) that prohibit those who have been disadvantaged from achieving their full health potential because of their social position or other socially and economically determine circumstances.
Where does Equity Washing come from?
More often that not, the barriers which are more statistically likely to keep some groups (e.g. by race, gender, income, ability, etc) from being able to achieve their full health potential are less of a reflection of the day to day choices a person makes and instead more of a direct reflection of decisions made by someone with more access to resources that limit access to the tools and resources needed to make that investment.
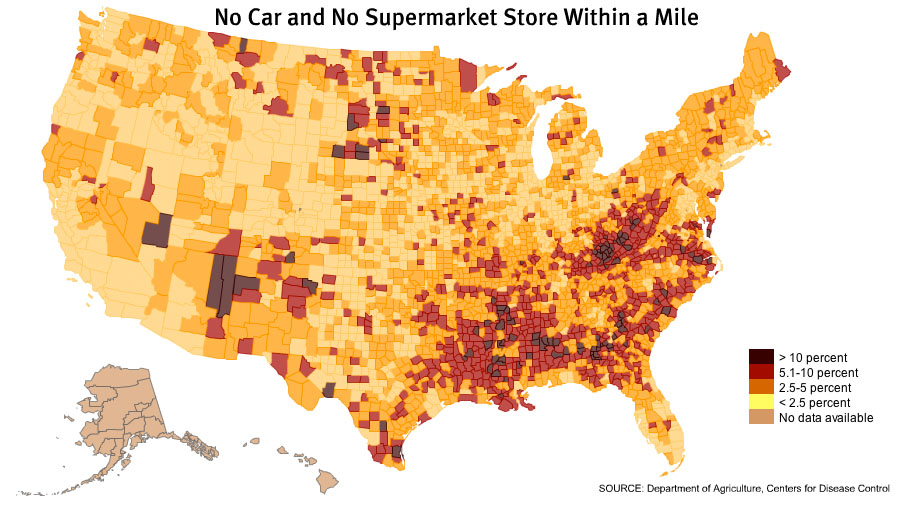
For example, in public health we use the example in which a low income person who receives a medical treatment becomes stigmatized by their medical provider about being overweight and recommends that the patient exercise more and eat more foods and vegetables.
Statistically, at a populations level, low income patients who experience obesity are more likely to live in a food desert, or an area where they have to travel more than a mile for access to fresh fruit and vegetables. The most available food they can afford may be from fast food restaurants and processed, nonperishable food or foods high in saturated fats from the local convenient store.
Image source: Jurgen Mantzke
In this case, a provider who claims to be equity-centered would not be engaging in equitable practices not just because they aren’t aware about the structural barriers which prohibit a person with limited access to healthy foods from being able to afford healthier choices. The provider would also fall within the framework of equity-washing, or promoting the concept of equity without engaging in the practice because they failed to listen to the experiences, needs, and preferences of the patient that may have helped them identify the root cause.
The failure to include the patient in the discussion and decision-making about their own clinical care not only created an impediment to appropriate intervention, it also provided a missed opportunity to connect the patient to social services or advocacy groups who could help that patient get access to appropriate care.
More frequently we see these kinds of dynamics play out is when public/private partnerships when speculator interests are used to pathologize and dispossess the impacted party of decision-making power under the guise that they aren’t educated enough to understand or their resistance is viewed as a direct threat to the benefits key decision-makers may gain from making a decision on behalf of those most directly impacted by a ‘bad faith’ decision.
Recently see these dynamics play out when this model is used to displace tenured urban residents from their communities for economic revitalization initiatives.
How is ‘Equity Washing’ Assessed?
While we may hear arguments that human being should be able to demonstrate free will and the capacity to make their own decisions, one way to truly determine whether a person has agency is by taking the time to evaluate:
Whether the Level of Agency initiated by the people DIRECTLY IMPACTED by the decision is whether:
the decision-maker has the power to set the agenda of the decision being made and participate fully in the the decisions which impact them
the decision-maker who is directly impacted by a decision hold sufficient power and authority to disagree or decline a decision without facing punitive consequences or having their input erased from the decision-making process
the decision can directly impact those who might face the consequences of a decision without their authorization or consent
Typically the level of contribution in the decision-making afforded to those directly impacted by decisions can provide a clear sense of whether a decision-making process is designed to repair harm or to replicate it.
When thinking through whether you or your organization may be approaching the decision-making process in a way that may not be equitable, it may be helpful to consider where your community engagement or governance model falls within the spectrum of equitable governance.
Level of Agency
How much authority does the decision-maker hold?
What level of contribution is permitted in the process of decision-making
no agency
holds no authority
decisions happen “to” versus “with”, often through political theater, force, or coercion
minimal agency
holds little authority
decisions happen “to” versus “with”, agent provided some opportunity to make informed/ albeit an uncertain level of choice
limited agency
holds little authority
consequences of decisions happen “to” AND “with”, agent provided some opportunity to contribute feedback regarding preferences but aren’t included in the decision-making
distributed agency
holds some weighted authority
decisions are made via consensus model but weight of decision-making authority is distrbuted unequally among decision-makers
cooperative agency
holds shared authority
decisions are made via consensus equally among decision-makers
equitable agency
concerns and preferences of those most impacted by a decision are prioritized
decisions are made centering the accessibility needs of those traditionally harmed by disparities in decision-making
full agency
time and resources are invested to ensure that those most impacted by a decision are prioritized have the information they need to provide informed consent to any decisions that affect them
informed decisions are made centering the accessibility needs of those most directly impacted with a clear understanding of the context and the opportunity to set the agenda for which options will be deliberated upon
This is the first installment of a five-part series on the origins of health disparities.
This stark image of disparity depicting a segregated bread line ‘At the Time of the Louisville Flood’ was taken in 1937 Photo credit:Margaret Bourke-White
Objectives
Upon completion of this post, participants will be able to:
Have a shared understanding to describe health and economic disparities
Understand how community resilience is different from property based systems of wealth
Have a shared language & mental map to measure whether their understanding of the role of public health and philanthropy is community-centered or based upon models that create/ replicate disparities in health
What are health disparities? | Defined
The term “health disparities” is often defined as “a difference in which disadvantaged social groups such as the poor, racial/ethnic minorities, women, disabled, and other communities that have persistently experienced social disadvantage or systemic discrimination to the point that they experience worse health or greater health risks than better resourced/more economically advantaged social groups.”[2]
Trigger warning:
This post includes an image of people who were enslaved to describe how disparities and extractive capital were used to create disparities in resources, dismantle democratic governance within communities, and shape the way we frame who is worthy of investment (and how that shapes community health )
Bhimbetka Petroglyphs, the earliest known cave paintings in human civilization (discovered in India during the 1990s)
The accumulation of tools, food, and the resources needed to sustain health were used to increase community resilience in the face of threats to their survival. Injuries, disabilities, and chronic illnesses were attributed to ancestral deities and spirits that could either be treated through rituals and the fate of those afflicted was considered beyond the control of the individual and their fate was surrendered in the hands of the spirits which governed the fate of the the those facing afflictions.
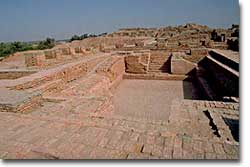
The “Great Bath” of Mohenjo-Daro is the earliest known public water tank of the ancient world. Most scholars believe that this tank would have been used in conjunction with religious ceremonies. Copyright: Copyright J.M. Kenoyer/www.harappa.co
Early agrarian societies formed as a way to better regulate the supply of surplus food storage to serve as a buffer against:
seasonal food scarcity and changing climates,
contaminated food supply, and
natural phenomena like plant disease and drought.
Because communities could shelter in place and store resources (e.g. food and tools) much longer, the prevalence of illness that originated from poor hygienic conditions and poor sanitation created the first public challenges among regional populations.
Emergence of disparities in access to capital
Seals such as these were used by merchants in the Harappan civilization. Photo courtesy of Carolyn Brown Heinz
As early humans expanded their knowledge of tools, land use, and animal domestication, those with the most favorable conditions or who controlled the most effective tools and knowledge for production found themselves with increased bargaining power in decision-making.
This created disparities in tools and knowledge.
This shift in accumulation of surplus value created an incentive for those who controlled capital to accumulate personal wealth.
Systems of commerce and land distribution also emerged to increase the productive capacity of property and expand wealth creation.
Emergence of hierarchal social structures & Disparate access to resources
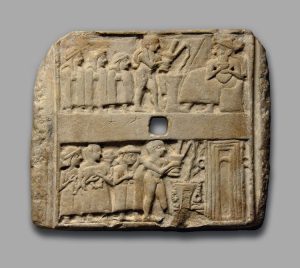
(Sumerian Artifact from one of the world’s earliest Mesopotamian civilizations kept at The British Museum, London). The upper register shows a naked priest followed by three worshippers. The priest pours an unknown liquid offering from a spouted vessel into a stemmed dish or stand, in front of a horned god figure. In the lower register, there are three worshippers; one of them carries an animal offering and one of them is a woman who is shown “full-faced.” She may be a priestess or she may represent the donor of the plaque. The priest’s libation is being poured in front of an unknown temple. The plaque was excavated at Ur, in the ruins of one of the residences of the high priestess of the moon god Nanna. Early dynastic period, circa 2500 BCE, from Ur, Mesopotamia, Iraq.
Those who, either experienced unfavorable growing conditions or encountered barriers to production, became much more reliant upon the benefactors who controlled resources like food, tools, and labor distribution for their survival and subsistence.
The labor force became another source of wealth for property owners. This fiscal value of human capital became measured by the costs used to maintain the force versus the revenues produced by their labor production.
This reduced the incentive of those who benefitted from these disparities to redistribute their resources and decision-making power in a way that was democratic or that prioritized the collective resilience and wellbeing of the community.
Those who controlled resources and capital were able to barter and negotiate for additional wealth, loyalty (and in many cases would steal under threat of coercion or violence) and the tools or expertise to make themselves more competitive than other members of their community through this concentration of wealth.
These shifts in incentive and power dynamics resulted not only in creating
systemic power imbalances,
the increase of infectious disease, and
fundamental shifts in the way we understand the role of bodily autonomy and consent in the labor force.
fundamentally shifted these communities relationship to one another, property ownership, and investment.
Property-Centered versus People-Centered communities
Society’s collective understanding of how power should be distributed became defined by those who held the most bargaining power, many of whom willfully asserted their claims to supremacy.
Knowledge, tools, and the extraction of human labor became much more commonplace.
This proprietary approach to capital created an incentive for property owners to develop strategies to control the supply of capital and create barriers to social mobility. Many of these efforts to suppress competition exposed those with less bargaining power to much higher risks of exposure to unsafe, unsanitary conditions.
These emerging hierarchal structures also shifted how narratives were framed regarding how merit is regarded and even went so far as to dictate whom would be considered worthy of dignity within the power structure.
Consequently, Accumulated and inherited wealth, or the ability to contribute toward property owners’ accumulation of wealth became the key metric for merit.
Many of these strategies even went so far as to create systems of wealth and property ownership using mechanisms like systems of forced labor, taxation, and debt.
Those who sought to keep and expand their status created narratives that attributed their fiscal advantages to royal supremacy and divine right, to dissuade subordinates from rebellion.
Often these messages were accompanied by violent and forceful indoctrination or state sanctioned practices of exclusion.
Property owners were granted authority over decision-making, and often chose to prioritize their commercial interests over the needs of the community.
Laborers who were most impacted were not granted the opportunity to share in the decision-making, but rather experienced the impact of those decisions. In many cases they were even deprived of resources or publicly humiliated when they expressed dissent with those decisions
There were often many cases in which dissenters perspectives were violently suppressed when they openly resisted despots and property owners.
Labor control systems, militaries, and were developed to coerce subordinates and the labor force into compliance.
These resulting trend of territorialism, socio-political suppression, and normalization of extractive, supremacist structures often resulted in the loss of communal knowledge, traditions, and inter-generational support.
We see patterns of this mindset replicated throughout colonial history as land acquisition and involuntary labor were used to establish criteria for who we believed was worthy of merit and who deserved to be subservient or poor.
This disturbing photo was taken in Lubo, Belgian Congo – November 14, 1924 to illustrate the history of Belgian colonialism in the Congo. Photo credit: Dispatch Press Images
How do disparities in wealth creation shape the way we measure merit and health?
Property ownership fundamentally shifted the way early civilizations shaped our current understanding of community health. This production model, also known as the extractive capital framework shifted the prioritization of the well-being and resilience of communities toward a model in which those with less resources were forced to collaborate or scheme to convince those who control the most resources that their needs and interests were WORTHY of the investment.
Reflect:
How does your understanding of power, and the way it is distributed, impact the way you approach power distribution in your own community or organization?
We often see disparities or statistical trends where people of different genders, ethnicities, and abilities don’t have the same access to financial stability, decision making or health outcomes.
But these disparities didn’t just happen in a vacuum.
They are often the result of specific policies or widespread institutional practices that create these inequalities.
What are racial disparities?
The term “health disparities” is often defined as “a difference in which disadvantaged social groups such as the poor, racial/ethnic minorities, women and other groups who have persistently experienced social disadvantage or discrimination systematically experience worse health or greater health risks than more advantaged social groups.”[2] When this term is applied to certain ethnic and racial social groups, it describes the increased presence and severity of certain diseases, poorer health outcomes, and greater difficulty in obtaining healthcare services for these races and ethnicities. When systemic barriers to good health are avoidable yet still remain, they are often referred to as “health inequities.”[3]
Why Bring Up Racial disparities?
In the United States, like many industrialized nations shares a history in which European colonists immigrated and seized property from indigenous populations in order to generate wealth for European property owners but restricted wealth building opportunities for people of other ethnicities with policies and practices designed to limit competition from other populations.
More importantly, these policies and practices were structured in such a way that prohibited non-white Europeans from making decisions about their own health, civil liberties, or living conditions. The policies also provided white property owners and post war veterans a financial and educational wealth-building advantage during the same period these policies were enacted to create disparities. Any advances or successful efforts to shift policy to create a more equal society in which everyone has the opportunity to build free and healthy lives has been undermined by those who have benefitted from these disparities through policies like (redlining, urban renewal, Nixon’s deregulation and shift toward a debt based monetary system, mass incarceration, gentrification, etc).
The choices made by these policy makers throughout United States history have created stark differences in wealth and health outcomes.
In 2016, the Institute for Policy Studies (IPS) and the Corporation For Economic Development (CFED) released the findings of a study in which they investigated trends in household wealth over a 30-year period and found that without ‘significant policy interventions, or a seismic change in the American economy,’
If current economic trends continue, the average black household will need 228 years to accumulate as much wealth as their white counterparts hold today. For the average Latino family, it will take 84 years.
The research showed that the average wealth of white households increased by 84 percent between 1983 to 2013, which was three times the gains that African-American families saw and 1.2 times the rate of growth for Latino families.
Coincidently, significant disparities in health resulting from disparities in access to care resulted in a similar trend among census tracts that experienced these wealth disparities.
While faulty cultural narratives that attempted to pathologize (or stereotype and stigmatize) communities of color for these outcomes, the realities these communities face was much more a byproduct of this long history of political and social apartheid than could be attributed to individual behaviors.
While factors like poverty, unemployment, and unhealthy health behaviors were assumed to be the product of poor moral or cognitive capacity to make better decisions, public health researchers began to use epidemiological surveillance methods to investigate the root causes for these health disparities.
What they found was that many of the communities that faced these health disparities were concentrated in census tracts with low homeownership and limited access to resources due to how cities were zoned and disparities in hiring and lending practices.
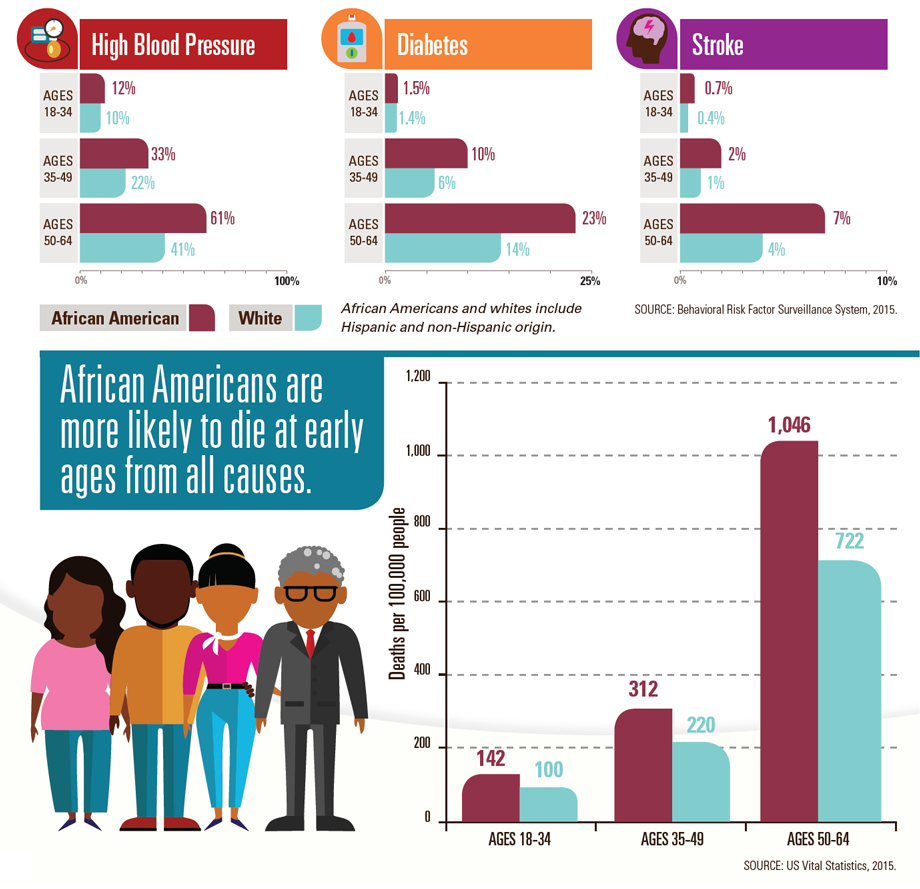
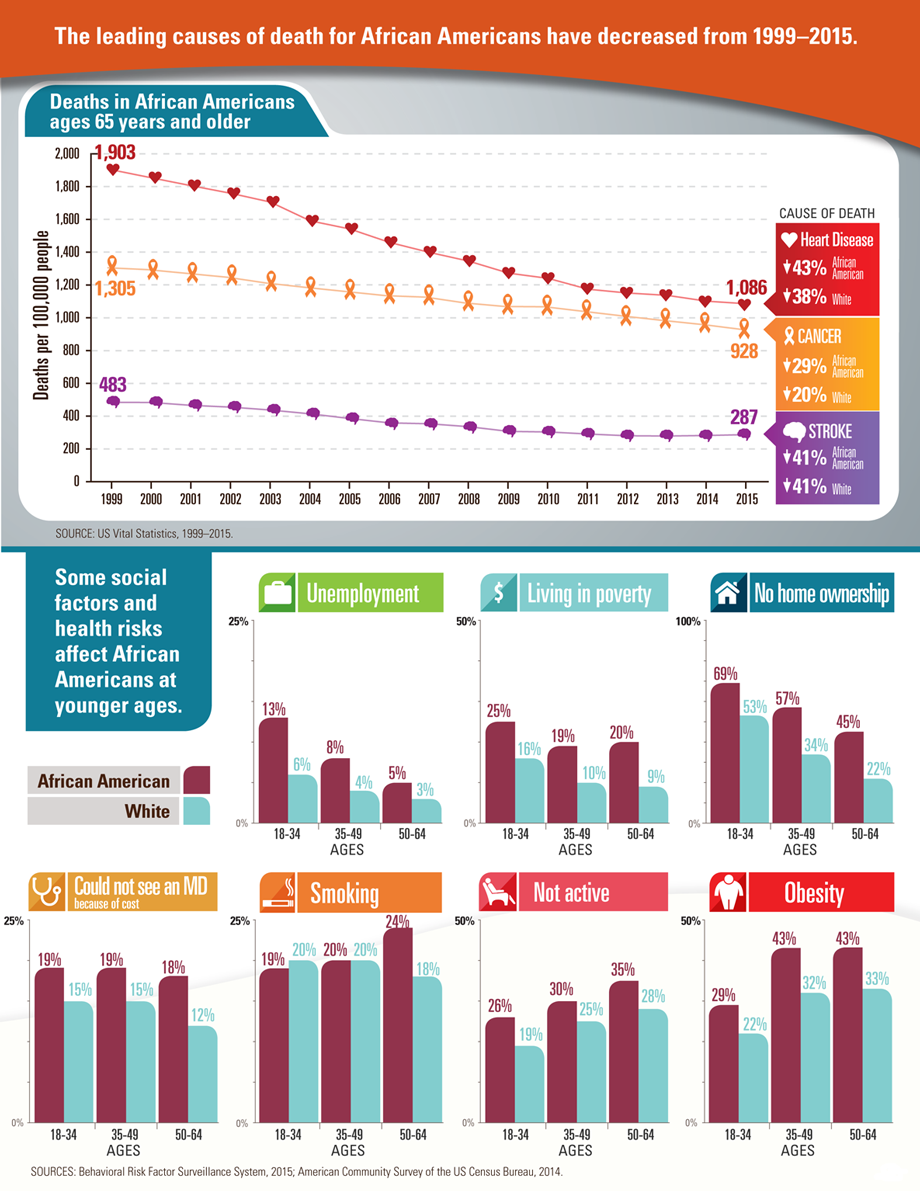
Residents in these census tracts who experienced higher rates of obesity, hypertension, and diabetes were significantly less likely (statistically) to have access to safe affordable food, were more likely to live in contaminated housing or to experience violence in their neighborhoods (by both law enforcement and from vigilante groups who took retaliation into their own hands rather than risk being placed into a victim/offender relationship with law enforcement), and were also less likely to earn the revenue or secure loans to get their basic needs met, let alone for high ticket costs like healthy housing, transportation, or childcare.
Whereas previous generations of black and brown immigrant families were able to pool resources and use tools like public housing and food assistance programs that were initially designed to help white working class workers save up enough money to purchase homes with government subsidies, which was the origin of much post-war middle class wealth.
Deregulation policies which ended the savings and loan model and government subsidies initiated by Nixon changed the monetary system in which wealth was transferred and how that distribution was concentrated. Families who could access to loans were expected to borrow loans and pay installments over long periods of time in order to create wealth using interest payments and stock dividends for the property owners and regulators who already had access to homeowner equity and other forms of pre-existing wealth.
Nixon’s War on Drugs criminalized black and brown communities for narcotics consumption and distribution, even though the primary source of drugs entering the country came through the military and medical system. The mass incarceration of black and brown communities created additional barriers to social mobility resulting in hiring and voting restrictions.
But the historic disparities didn’t just harm the black and brown folks who consumed controlled substances. The effects of these regulations and practices also replicated disparities among members of these communities who did their best to assimilate into a monetary system that wasn’t designed to include them.
In 2018, the research team led by Dr. Willian Darrity and Darrick Hamilton that investigated whether African Americans who:
invested in higher educational attainment
invested in homeownership
purchased and banked from an investment pool concentrated predominantly within the black community
What their study did was debunk many myths and narratives that had been used to discredit the efforts of communities that had experienced racial and financial apartheid
So how do we repair it?
Click to learn more about the role of Equity in ending racial disparities.
By request, I will be developing content for a post about an assessment rubric I wrote on ‘Equity Washing.’
In order to understand what equity. washing is, we first need to define what Equity IS and ISN’T.
What is Equity?
In the field of public health,
“Health Equity is the measurable standard by which every person has the opportunity to “attain his or her full health potential” and no one is “disadvantaged from achieving this potential because of social position or other socially and economically determined circumstances.”
— C E N T E R S F O R D I S E A S E CO N T R O L
The World Health Organization and Centers for Disease Control measure health equity using sets of risk factors that describe how upstream risk factors: (e.g.
macroeconomic policies
historical roots of inequities
systemic power imbalances, and
combine with:
hereditary or developmental factors
economic status, educational attainment
place of residence (urban/rural), subnational region, and health behaviors)
to shape life expectancy, mortality, and other disease burden indicators that might statistically shape a person’s quality of life throughout their life course.
This means that if a person’s life experiences followed the same trends we see statistically at populations level (or trends we see that cluster in units of 100,000 people across many communities) that reflect the trends we see in people who shared their hereditary and economic circumstances, the person would be statistically more likely to have health outcomes consistent with the regional trend unless a policy or institutional intervention changes their life course.
We often see disparities or statistical trends where people of different genders, ethnicities, and abilities don’t have the same access to financial stability, decision making or health outcomes.
But these disparities didn’t just happen in a vacuum.
They are often the result of specific policies or widespread institutional practices that create these inequalities.
For example, in:
Racial disparities
In the United States, like many industrialized nations shares a history in which European colonists immigrated and seized property from indigenous populations in order to generate wealth for European property owners but restricted wealth building opportunities for people of other ethnicities with policies and practices designed to limit competition from other populations.
In the United States, like many industrialized nations shares a history in which women were prohibited from owning or managing property or asset related decisions without permission of their parents or husbands. The United States also shares a history of violence against gender nonconforming communities that often results in discrimination and exposure to violence.
[Stay Tuned for my upcoming post about how Gender Disparities shape Health Disparities]
Disability disparities
In the United States, like many industrialized nations shares a history in which people with cognitive and developmental impairments were prohibited from making decisions about their own access to healthcare or living conditions.
[Stay Tuned for my upcoming post about how Ablelism shapes Health Disparities]
What is the role of Equity in repairing health and economic disparities?
These policy level, economic, and epidemiological studies, used populations level evidence and an empirical, peer reviewed methodologies to demonstrate how this history of apartheid, and the people who benefit from the disparities formed by these policies and practices have a direct responsibility to repair the harm they have and will cause to many generations to come.
While many of our policy and philanthropic models used to provide assistance to vulnerable populations are built upon outdated narratives that attribute these disparities to ‘a lack of will’ or ‘moral failure’ rather than acknowledge and dismantle the structural disparities.
The principles of equity call upon communities to share ownership and investment in the repair of this deep, systemic structural harm prioritizing the needs of those most in need or crisis so that they have access to the resources they need to build resilience (in a way that’s trauma informed and community led).
Consequently, many policy makers and philanthropic funders who express a desire (often in the form of a spoken or written commitment) to invest in this structural repair either have little knowledge of this history and use a ‘deserving poor’ approach to investment, or take so much ownership of dictating how repair should happen that they end up replicating many of the systemic harms and practices that harmed these communities and exclude communities that have been harmed from the decision-making process. This is more often than not predicated on the basis that these gatekeepers:
aren’t aware how they replicate supremacist power dynamics
pathologize these communities and don’t trust these communities to advocate for themselves
see criticism from these communities as something to be defensive or resentful about rather than an opportunity to collaborate or support those who are closest to these challenges
So how do we repair it?
Stay tuned for more information addressing many of the strategies we can use to share ownership and investment in repairing these systemic harms.
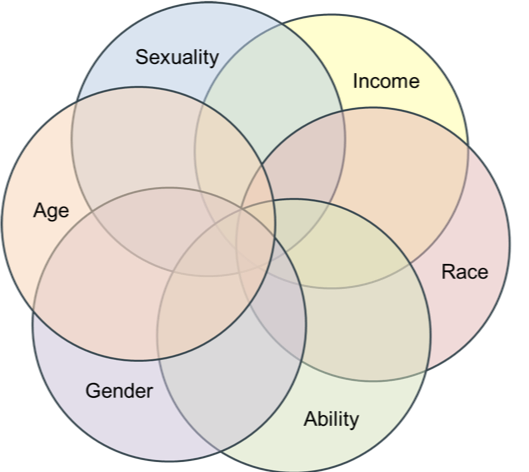
“the complex, cumulative way in which the effects of multiple forms of discrimination (such as racism, sexism, and classism) combine, overlap, or intersect especially in the experiences of marginalized individuals or groups.”
Where did the word come from?
The term intersectionality was actually coined by Kimberlé Williams Crenshaw, one of the attorneys who assisted the legal team representing Anita Hill at the U.S. Senate confirmation hearings for Supreme Court Justice Clarence Thomas. Crenshaw is much more known for her work as a legal scholar who works to prevent race and gender violence and the courses she teaches as a professor at UCLA in the following specializations:
Advanced Critical Race Theory;
Civil Rights;
Intersectional Perspectives on Race,
Gender and the Criminalization of Women & Girls; and
Race, Law and Representation
She also has a podcast called Intersectionality Matters.
How is the concept of intersectionality used?
Excellent question!
In public health, intersectionality is used to explain why the health of one group of people in the community may be different than the health of someone who shares similar characteristics.
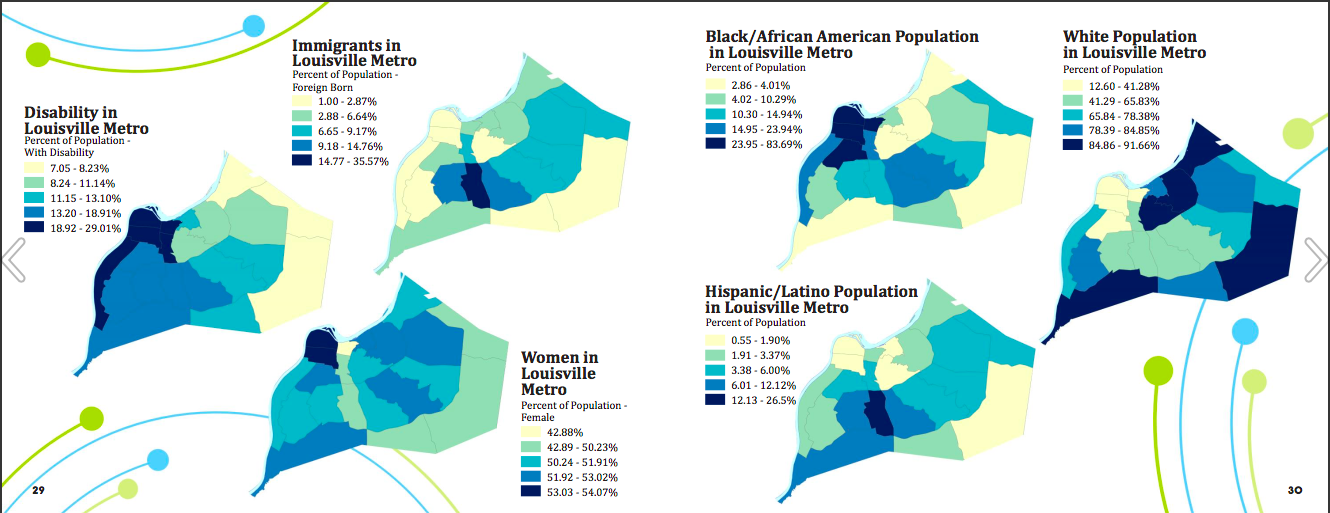
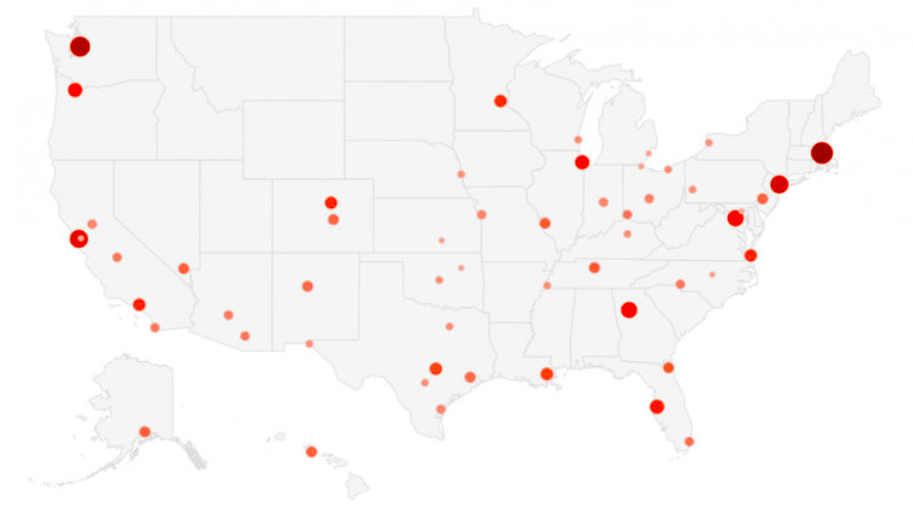
Image of demographic information reflected in geospatial maps from Louisville KY’s healthequityreport.com
For example, if you wanted to find out whether black women with disabilities are more likely to die in childbirth than we would expect for the maternal life expectancy rates of all women in a specific geographic area, you could use census information to find out what the rate was for black women, for women with disabilities, for all women.
But it wouldn’t help us be able to understand whether the experiences are different or similar for each of these populations.
Intersectionality helps us to plan and structure the way we look at information to measure and assess all of these types together so that we can work with more accurate information.
Discuss
In the comments below, describe ways you’ve used the concept of intersectionality to inform YOUR work.














 The ownership and concentration of wealth, knowledge, and bargaining power shifted the way societies were structured that transformed communities from being resilience centered toward
The ownership and concentration of wealth, knowledge, and bargaining power shifted the way societies were structured that transformed communities from being resilience centered toward